When you click on links to various merchants on this site and make a purchase, this can result in this site earning a commission. Affiliate programs and affiliations include, but are not limited to, the eBay Partner Network.
From: Mid-Atlantic (on land, not in the middle of the ocean)
Originally Posted by Mahler9th
I think folks may still feel that the sleep study report somehow "confirms" that CPAP is no longer needed or recommended, and that PCA/PCA CR must realize that after a careful review.
I don't think that is the case.
This relates to the first paragraph in the letter the OP received from PCA CR and posted in this thread.
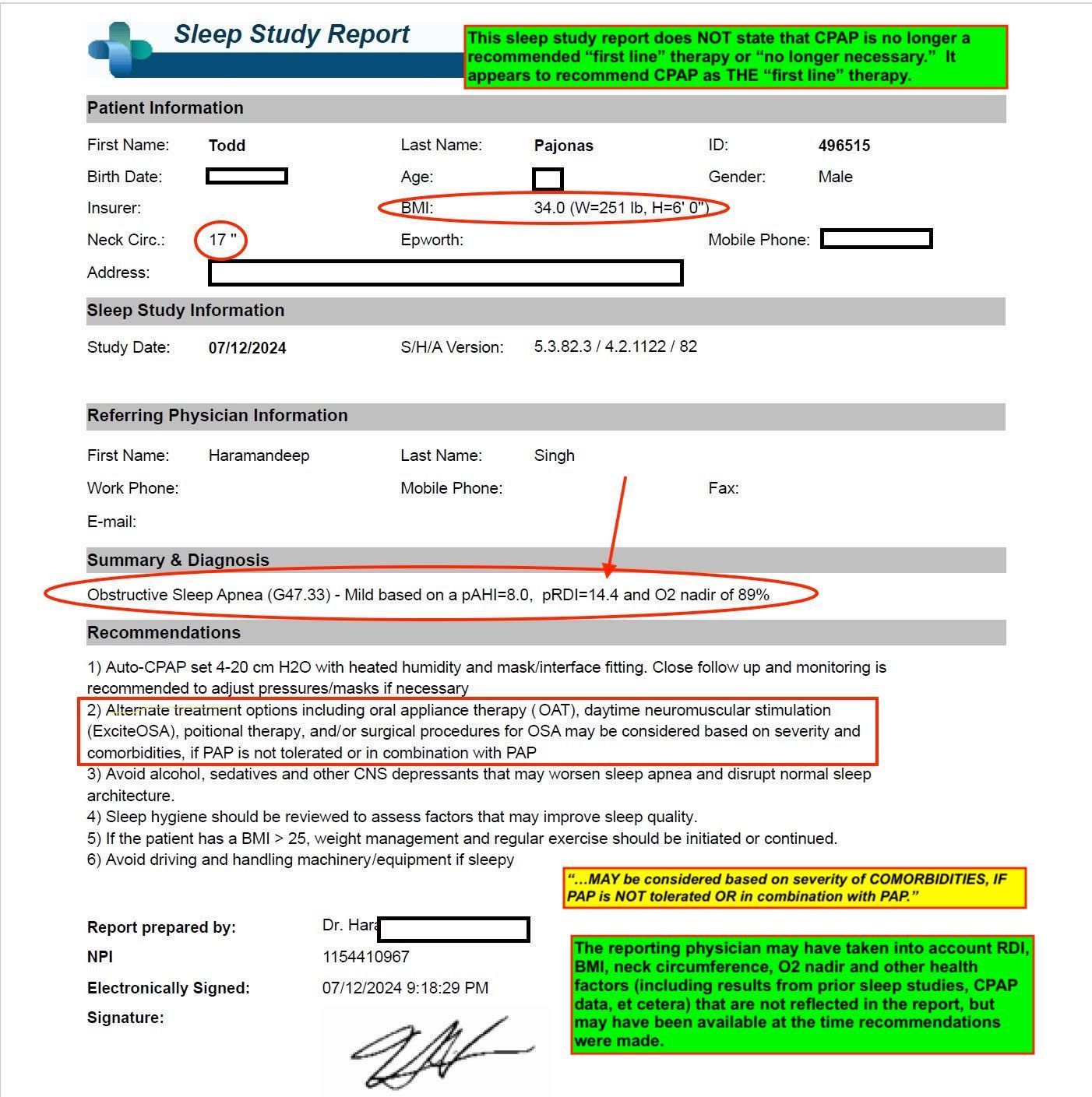
This sleep study report does NOT state that CPAP is no longer a recommended “first line” therapy or “no longer necessary.” It appears to recommend CPAP as THE “first line” therapy.
The reporting physician may have taken into account RDI, BMI, neck circumference, O2 nadir and other health factors (including results from prior sleep studies, CPAP data, et cetera) that are not reflected in the report, but may have been available at the time recommendations were made.
I think that it is possible that if the reporting physician had written a summary letter that stated that he or she believed the OP's ability to race with OAT is sufficient, and this letter was provided to PCA CR, then PCA CR may have written a different first paragraph.
Folks should realize that "CPAP data," may not be so simple as one might initially believe. In the context of PCA CR, according to the OP, what is requested is "compliance data."
That is information shows usage-- and as I have stated before, it appears that:
1. In trucking, one suggested threshold is 90 nights of data, showing at least four (4) hours of use for 70% of nights. One might guess that the certified examiners have SW tools to take raw data and yield a "yes or no" answer to this, but it seems clear that those examiners have some "authority" to look at other health factors in making their determinations.
2. Again, it seems clear that in trucking, examiners have all kinds of flexibility for situations where a candidate's level of OSA has led to CPAP rx, but the candidate does not have 90 days worth of data to provide.
I hypothesize that all of this OSA/CPAP activity in trucking was in part catalyzed by the emergence of commercially available home sleep testing capabilities-- perhaps more so by that than the terrible accident that injured Tracy Morgan and the resulting litigation.
In any case:
1. I encourage the OP to make careful decisions regarding current and future OSA rx.
2. I encourage PCA CR to re-think its approach to OSA as it relates to licensure.
I think that report is somewhat ambiguous. If I was the patient, I would need to ask the doctor to clarify. The report doesn't say that CPAP is no longer needed, and sort of implies that it is needed, but it's not clear whether use of the treatments on the second line would make it unnecessary to use the CPAP.
Mahler you need to stop trying to diagnose me when you don't have all the relevant facts.
Firstly, when there is a sleep score of 8, which is what I have, a CPAP machine is not called for. Why did they add that recommendation? Because sleep studies are a BUSINESS and they want to sell me a CPAP machine. If you read medical journals on OSA they do not require CPA treatment for my level of OSA.
In addition, you keep citing BMI and neck size. Those are contributing factors to OSA, they are not reasons alone to use a CPAP. Your conclusions along those lines are specious. I monitor my sleep both with a smart watch, and several times a month, a pulse oximeter. I am concerned about my health, and since I am not longer going to race with PCA, I don't need to not use a CPAP. It doesn't make a difference. The reality is I really don't need it anymore.
I also think it was pretty obnoxious of you to render a diagnoses that I do tolerate the CPAP. I was very fortunate for years that I was able to tolerate the mask, but what I always struggled with was a rash under my nose. I tried all different manufacturers of the appliance as well as creams. The reality was, once a rash started it would only get worse to the point I sometimes had cracked skin under my nose and looked like I did coke or had a really bad cold. Who the hell are you to say this wasn't a problem for me? It caused great discomfort when I was trying to sleep. Accordingly, since the CPAP is not well tolerated, I can use an oral appliance.
Throughout this whole process I have not minded people taking an opposite view - everyone is entitled. But as the saying goes, you are entitled to your opinion, but you are not entitled to your own facts, and many things you are pawning off as fact are in fact your opinion. You're just plain wrong.
If you want to state an opinion that's fine, but please stop it with this professor bull**** where you just misinterpret everything to be contrary. This is exactly what PCA does and you are making yourself look just as foolish.
Last edited by LuigiVampa; 08-20-2024 at 03:27 PM.
I wasn't going to bring this up, but I was recently tested for sleep apnea and the results came back as borderline. When speaking with the medical professional who walked me through the squiggly lines, she revealed that my score would allow me to be eligible for treatment, if I wanted it, but not necessary in my case. Ironically enough, she let slip that if I was on Medicare, my score would not be considered "borderline" and would not be eligible for treatment. Bottomline is that the confirmation or absence of my sleep apnea came down to how I was insured, if I'm on private insurance, I had sleep apnea, if on Medicare, I did not.
Mahler you need to stop trying to diagnose me when you don't have all the relevant facts.
Firstly, when there is a sleep score of 8, which is what I have, a CPAP machine is not called for. Why did they add that recommendation? Because sleep studies are a BUSINESS and they want to sell me a CPAP machine. If you read medical journals on OSA they do not require CPA treatment for my level of OSA.
In addition, you keep citing BMI and neck size. Those are contributing factors to OSA, they are not reasons alone to use a CPAP. Your conclusions along those lines are specious. I monitor my sleep both with a smart watch, and several times a month, a pulse oximeter. I am concerned about my health, and since I am not longer going to race with PCA, I don't need to not use a CPAP. It doesn't make a difference. The reality is I really don't need it anymore.
I also think it was pretty obnoxious of you to render a diagnoses that I do tolerate the CPAP. I was very fortunate for years that I was able to tolerate the mask, but what I always struggled with was a rash under my nose. I tried all different manufacturers of the appliance as well as creams. The reality was, once a rash started it would only get worse to the point I sometimes had cracked skin under my nose and looked like I did coke or had a really bad cold. Who the hell are you to say this wasn't a problem for me? It caused great discomfort when I was trying to sleep. Accordingly, since the CPAP is not well tolerated, I can use an oral appliance.
Throughout this whole process I have not minded people taking an opposite view - everyone is entitled. But as the saying goes, you are entitled to your opinion, but you are not entitled to your own facts, and many things you are pawning off as fact are in fact your opinion. You're just plain wrong.
If you want to state an opinion that's fine, but please stop it with this professor bull**** where you just misinterpret everything to be contrary. This is exactly what PCA does and you are making yourself look just as foolish.
Specious? Oximeter?
You've going too far here. Where's the love Luigi? You should be a bit more greatful to me....
I wasn't going to bring this up, but I was recently tested for sleep apnea and the results came back as borderline. When speaking with the medical professional who walked me through the squiggly lines, she revealed that my score would allow me to be eligible for treatment, if I wanted it, but not necessary in my case. Ironically enough, she let slip that if I was on Medicare, my score would not be considered "borderline" and would not be eligible for treatment. Bottomline is that the confirmation or absence of my sleep apnea came down to how I was insured, if I'm on private insurance, I had sleep apnea, if on Medicare, I did not.
Wait, what? I have private insurance, Does that mean I should get a CPAP machine?
Mahler you need to stop trying to diagnose me when you don't have all the relevant facts.
Firstly, when there is a sleep score of 8, which is what I have, a CPAP machine is not called for. Why did they add that recommendation? Because sleep studies are a BUSINESS and they want to sell me a CPAP machine. If you read medical journals on OSA they do not require CPA treatment for my level of OSA.
In addition, you keep citing BMI and neck size. Those are contributing factors to OSA, they are not reasons alone to use a CPAP. Your conclusions along those lines are specious. I monitor my sleep both with a smart watch, and several times a month, a pulse oximeter. I am concerned about my health, and since I am not longer going to race with PCA, I don't need to not use a CPAP. It doesn't make a difference. The reality is I really don't need it anymore.
I also think it was pretty obnoxious of you to render a diagnoses that I do tolerate the CPAP. I was very fortunate for years that I was able to tolerate the mask, but what I always struggled with was a rash under my nose. I tried all different manufacturers of the appliance as well as creams. The reality was, once a rash started it would only get worse to the point I sometimes had cracked skin under my nose and looked like I did coke or had a really bad cold. Who the hell are you to say this wasn't a problem for me? It caused great discomfort when I was trying to sleep. Accordingly, since the CPAP is not well tolerated, I can use an oral appliance.
Throughout this whole process I have not minded people taking an opposite view - everyone is entitled. But as the saying goes, you are entitled to your opinion, but you are not entitled to your own facts, and many things you are pawning off as fact are in fact your opinion. You're just plain wrong.
If you want to state an opinion that's fine, but please stop it with this professor bull**** where you just misinterpret everything to be contrary. This is exactly what PCA does and you are making yourself look just as foolish.
You are now being an even bigger J**k.
I have NOT tried to diagnose you. Not in any way, shape or form.
YOU have tried to diagnose yourself.
Based on what I have read in your post, I believe my understanding of these matters exceeds yours, and based on my educational, professional and personal background, and what I can assume of yours, that is no surprise.
Parameters like BMI and neck circumference are NOT SIMPLY!!! "contributing factors to OSA."
There are ALSO!!! PERHAPS!!!, parameters that are considered by HCPs in determining diagnoses AND or rx recommendations.
As I have stated before, a single AHI number from a single study MAY NOT be sufficient to determine whether CPAP rx is appropriate either initially or a continued basis.
When you incessantly insist otherwise in communications with PCA CR folk that are medical professionals, especially after all that has transpired, you may not be putting your best foot forward.
In fact you may look like a complete (expletive deleted).
Human physiology is complex, and dx and rx for things like OSA are as well.
On the personal side...
I took great pains to explain this to someone who struggled with OSA for years and had two sleep studies which resulted in the ENT failing to prescribe CPAP rx.
The studies were ordered by a well-trained and expert ENT. When he initially physically examined the patient, he was SURE that a sleep study would provide results (NOT just AHI score) that would "justify" CPAP rx. This was a Sutter Health ENT (the board chairman of which at the time was a local PRC/PCA racer).
IIRC, the AHI numbers were under 10. I never reviewed the full reports.
I saw the patient continue to struggle for years. The untreated OSA was extremely debilitating, but she considered the study results "black and white," just like other laypersons might.
Of course this person was able to drive a high demand Porsche race car near its limits without falling asleep. Same person achieved TTOD at a PCA GGR TT event.
Finally the patient agreed to have another study. A 5-6 year period had elapsed. Same practice, different ENT and different sleep lab. AHI of 29.
Within two weeks CPAP therapy started and was life changing.
Winders and Nowanker know the person to which I refer.
On the professional side...
My training is in electrical and biomedical engineering, and during my graduate studies I took several pre-med courses, including a course in medical physiology. During college and grad school I worked for GE Healthcare in engineering roles. After grad school I went to work on the business side in medical device and equipment companies that made and sold products for dx and rx. Management.
In the first few months of my first job out of engineering grad school, I gave grand rounds to the radiology department at Columbia Pres.
I have worked with many kinds of doctors, and many kinds of attorneys. I have worked on this biz side to present safety and efficacy data to FDA and FDA advisory panels for clearances and pre-market approvals.
Folks that first successfully commercialized things like pulse ox, CT, MRI, CPAP are one degree away in my NW.
I have been a part of "corporate efforts" that have not soley targetted HCPs and healthcare business professionals, but also consumers.
Ask me about the GlucoWatch.
Ask me about aesthetic medical procedures and equipment.
And governments... ask me about infant hearing screening.
You state:
"...sleep studies are a BUSINESS and they want to sell me a CPAP machine. If you read medical journals on OSA they do not require CPA treatment for my level of OSA.."
Intersection of business and medical/healthcare.
I likely have a bit more experience on the topic of than you... ask me about renal lithotripsy some day.
Or radiology self-referral in the early days of CT and MRI.
When you insist that an AHI score of 8 from a single sleep study should prove to PCA CR or anyone else, that you no longer need CPAP rx, you may be mistaken.
As I am sure you can conclude from my posts, I disagree with what has apparently been done by PCA CR on this topic.
And of course you can draw your own conclusions about "standards of care" for OSA.
But I feel compelled to at least suggest to others whom may read this thread that OSA diagnosis and recommendations for therapies MAY not be as simple as a single sleep test and a single parameter, AHI.
This perspective may help a reader of this thread, or someone they care about.
It has NOTHING to do with racing in a PCA CR.
The same is true for blood glucose levels and A1C for folks with diabetes.
From: Formerly the DPRK, now seeking political asylum in Oregon
Originally Posted by multi21
I wasn't going to bring this up, but I was recently tested for sleep apnea and the results came back as borderline. When speaking with the medical professional who walked me through the squiggly lines, she revealed that my score would allow me to be eligible for treatment, if I wanted it, but not necessary in my case. Ironically enough, she let slip that if I was on Medicare, my score would not be considered "borderline" and would not be eligible for treatment. Bottomline is that the confirmation or absence of my sleep apnea came down to how I was insured, if I'm on private insurance, I had sleep apnea, if on Medicare, I did not.
What?!
You didn't disclose your borderline OSA?!
Lying on your license application?!
No soup for you!
I wasn't going to bring this up, but I was recently tested for sleep apnea and the results came back as borderline. When speaking with the medical professional who walked me through the squiggly lines, she revealed that my score would allow me to be eligible for treatment, if I wanted it, but not necessary in my case. Ironically enough, she let slip that if I was on Medicare, my score would not be considered "borderline" and would not be eligible for treatment. Bottomline is that the confirmation or absence of my sleep apnea came down to how I was insured, if I'm on private insurance, I had sleep apnea, if on Medicare, I did not.
Great illustration of the complexities involved...
"Bottomline is that the confirmation or absence of my sleep apnea came down to how I was insured, if I'm on private insurance, I had sleep apnea, if on Medicare, I did not."
Is that your conclusion? Or is that something the HCP stated?
Dx "should" be free of any consideration of reimbursement or coverage, but murkiness can sometimes result from less than ideal communication.
Might be beneficial to understand differences between "standards of care," and things like "first line rx," and "second line rx."
And how those things may differ from coverage/reimbursement.
One of my college classmates runs Anthem, and I am suspect they have a range of coverage/reimbursement criteria for things like CPAP rx.
If the patient told the HCP (e.g., sleep doctor) that he or she could simply not tolerate CPAP, and worked with the patient to pursue OAT...
This might be "charted," that is, made part of the patient's health record.
Now let's say this patient disclosed OSA and first line dx of CPAP to PCA CR.
And let's say the patient was told by PCA CR that they needed to provide a letter from the sleep doctor that states first line rx was not tolerated and that OAT was sufficient.
So the doctor looks at the chart and provides said letter to the patient and this letter is provided to PCA CR.
Different outcome?
"Suggestion" from the trucking space:
"Not all truck drivers with an apnea-hypopnea index greater than five (AHI > 5) may require treatment. Given the “no-rule rules,” FMCSA and CMEs generally agree that only moderate and severe sleep apnea (AHI > 15) rise to the level of a respiratory dysfunction likely to interfere with the ability to control and drive a commercial motor vehicle safely.
In general, AHI greater than five but less than 15 may not require treatment for FMCSA medical card purposes. In these cases, seeking the expert medical opinion of the M.D. interpreting the HST or doing a post-study consultation on treatment is important.
Having the M.D. chart state that “this patient does not have sleep apnea to the severity that it would interfere with their ability to drive a commercial motor vehicle in interstate commerce,” or something to that effect, is important. Similar language should be used with titration studies done to establish efficacy of treatment with the oral appliance (OA) if AHI less than five is not accomplished with the OA."
BTW, it appears that the study referenced in this thread was a titration study with CPAP.
Do you folks understand what that means?
Also "lessons?" from trucking:
"RC: Is continuous positive airway pressure (CPAP) compliance failure sufficient for a truck driver to qualify for oral appliance therapy?
BS: You can try, but as the “no-rule rules” apply, the CMEs have latitude in their certification decisions. The 2012, 2015 and recent Sept. 29, 2021, MRB discussions about using oral appliance therapy (OAT) for drivers have all concluded that it is not a first-line treatment option for truck drivers.
The MRB is not willing to certify drivers for OAT unless they have a documented CPAP failure. Presenting American Academy of Sleep Medicine (AASM) and American Academy of Dental Sleep Medicine (AADSM) current clinical practice statements on the topic has not changed this guidance. On many different conditions, treatment and efficacy requirements for CME certification are more restrictive than for the general public.
There are some cases where individual CMEs have certified drivers for OAT without a documented CPAP failure, but they are rare. If considering this as a treatment plan, confer with the driver’s CME in advance. Getting a second opinion from a different, more enlightened or OSA-aware CME may be needed." https://glidewelldental.com/company/...leep-apnea-osa


 08-20-2024 | 02:06 PM
08-20-2024 | 02:06 PM